Background
|
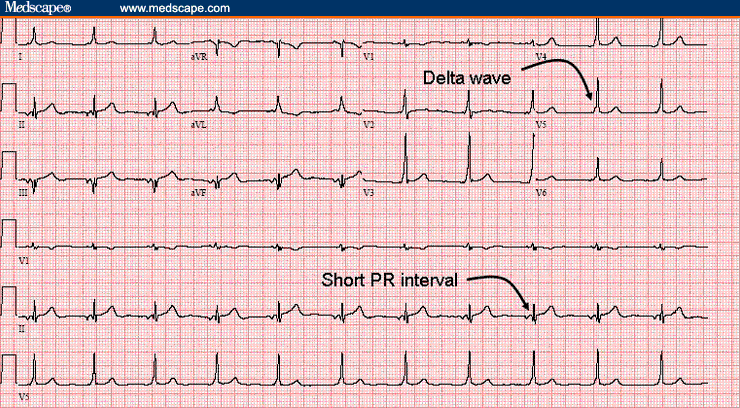
Figure 1. |
A 24-year-old man with no significant past medical history presents to the emergency department (ED) with a complaint of several episodes of a sensation of nearly blacking out. The episodes have occurred about 3-4 times over the 3 days before presentation. The duration of each episode has ranged from a few minutes to over an hour. The patient notes that he has felt his "heart beating really fast," with associated light-headedness. He denies having any chest pain, shortness of breath, or nausea associated with these events. He cannot identify exacerbating or alleviating factors; specifically, he denies exertion as an inciting factor. The remainder of his review of systems is negative except for some mild chronic shortness of breath. The patient takes no medications at home and has no active medical conditions. He smokes 2-4 packs of cigarettes per day and has done so for 5-6 years. He denies any illicit drug use or recent use of over-the-counter medications or herbal remedies. He has no history of any significant cardiac disease or sudden cardiac death in his family.
On physical examination, the patient is afebrile, with a pulse of 65 bpm, a blood pressure of 120/84 mm Hg, and a respiratory rate of 15 breaths/min. His room air saturation reading is 100%. In general, he is well-appearing and in no acute distress. The patient's neck examination shows no jugular venous distention. The heart sounds, including S1and S2, reveal no audible murmurs, rubs, or gallops. The apical impulse is nondisplaced and of normal impact. The lung sounds are diminished throughout, but there are no wheezes, rales, or rhonchi. He has no edema of the lower extremities, and the distal pulses are easily palpable. All other exam findings, including a neurologic examination, are unremarkable.
The patient is placed on a cardiac monitor, and an 18-gauge intravenous (IV) catheter is inserted into the antecubital fossa. Laboratory tests consisting of a complete blood count (CBC) and serum electrolytes are ordered. A portable chest radiograph reveals slight hyperinflation and hyperlucency of the lung fields, with a flattened diaphragm and central pulmonary artery enlargement. An electrocardiogram (ECG) is obtained (see Figure 1).
Discussion:
|
Figure 2. |
Preexcitation is characterized by an accessory pathway within the heart that conducts action potentials between the atria and ventricles outside of the normal conduction system (which conducts through the atrioventricular [AV] node-His-Purkinje system). The phenomenon was defined by Durrer et al in 1970, who stated that "preexcitation exists, if in relation to atrial events, the whole or some part of the ventricular muscle is activated earlier by the impulse originating from the atrium than would be expected if the impulse reached the ventricles by way of the normal specific conduction system only."[5] Of the various types of preexcitation syndromes, the most common is Wolff-Parkinson-White (WPW) syndrome.
WPW syndrome can be identified by a classic fusion QRS complex ECG pattern that is a combination of simultaneous normal conduction through the AV node and aberrant conduction through the accessory tract. This fusion QRS complex leads to particular ECG features that include a shortened PR interval (<120 msec) and a widened QRS complex with a delta wave representing preexcitation of the ventricle through the accessory pathway. The distinctive ECG pattern of the accessory pathway was initially described by Wolff, Parkinson, and White in 1930 as a bundle branch block with a short PR interval. Additionally, as mentioned, WPW syndrome is recognized as the most common form of ventricular preexcitation, although it likely represents a collection of pathologic conditions rather than a single structural abnormality.
Normal cardiac conduction of action potentials from the atria to the ventricles occurs exclusively through the AV node; the atrial impulses are subsequently propagated through a specialized conduction system (the AV-His-Purkinje system) and finally terminate in the ventricular myocardium. Action potential conduction through the AV node depends on slow inward calcium currents. In addition, the AV nodal system exhibits decremental conduction, which provides a protective effect; as the cardiac cycle is shortened (eg, the heart rate increases), there is decreased conduction through the AV node. This phenomenon limits the ventricular response to rapid atrial rates, such as those observed in atrial fibrillation or atrial flutter.
In preexcitation syndromes such as WPW, however, the action potential conducts to the ventricles at least partially through an accessory pathway termed the AV bypass tract or the bundle of Kent. Action potential propagation in the accessory pathway in WPW syndrome occurs through a rapid cellular influx of sodium. The consequence of the sodium-dependent action potential propagation mechanism is an accelerated conduction of impulses by the accessory bypass tracts, which leads to early activation of the ventricle as demonstrated by a shortened PR interval and a "slurred" QRS complex (ie, delta wave). Ventricular depolarization slowly spreads out from the bypass tract, while normal conduction that has been somewhat delayed through the AV node begins to conduct through the His-Purkinje system and spreads quickly to the remaining ventricular musculature. Although conduction velocity through the accessory pathway is faster than it is through the AV node, the accessory pathway often has a longer refractory period and, as such, is slower to recover excitability. Interestingly, the conduction of action potentials through the accessory pathway is nondecremental; therefore, the protective effect achieved by the AV node at higher heart rates is lost. These differences have important clinical implications. For example, a premature beat may conduct through the AV node normally while the accessory pathway remains refractory to conduction. The impulse then travels in a retrograde direction through the accessory pathway after ventricular depolarization, when it has recovered excitability. The consequence of this is the propagation of a reentry loop termed an orthodromic AV reciprocating tachycardia. This can then lead to rapid ventricular response rates that can degenerate into ventricular tachyarrhythmias. Rarely, antidromic tachycardias occur; conduction occurs in an anterograde direction through the accessory pathway and in a retrograde direction through the AV node.
Ventricular depolarization occurs through both the AV node-His bundle pathway and the accessory pathway; each pathway affects the ventricles by various degrees, depending on their relative activation times. As AV nodal conduction is delayed by either rapid atrial pacing or premature atrial beats, the accessory pathway contributes to a greater degree, resulting in a wider QRS morphology with an increasingly slurred delta wave. If the relative conduction time through the AV node is sufficiently delayed, total activation of the ventricle may occur through the accessory pathway.
The presence of accessory bypass tracts is not uncommon in the general population; however, less than half of the people with bypass tracts actually sustain a tachyarrhythmia. WPW syndrome affects approximately 0.15-0.2% of the general population, and of these individuals, 60-70% have no other evidence of heart disease. Mortality and morbidity associated with WPW syndrome occur as a result of associated dysrhythmias or from mistreatment of these dysrhythmias with inappropriate medications. Most studies report that the incidence of sudden death is in the 0-4% range. Men are affected more often than women,[5] accounting for 60-70% of all cases. Although this disease affects people of all ages, it is typically first recognized in children and young adults who present to the ED or their primary care physician with symptoms secondary to a dysrhythmia. Genetic mutations have been identified (by mapping genetic defects to specific loci) that account for the increased incidence of WPW syndrome in certain families.[2]
In patients with suspected WPW syndrome, evaluation should initially be directed at confirming the diagnosis and recognizing any potentially life-threatening arrhythmias. In patients with life-threatening arrhythmias, direct-current cardioversion should be immediately administered. In stable patients with tachyarrhythmias, an antiarrhythmic medication may be administered to terminate the arrhythmic episode, rather than immediately performing electrical cardioversion.
Studies have demonstrated that the best and most cost-effective treatment for patients with asymptomatic WPW syndrome is simple observation.[5] Most patients with symptomatic arrhythmias, drug-refractory WPW syndrome, or significant life-threatening arrhythmias are treated with nonpharmacologic therapy. Surgical ablation, previously the standard technique for drug-refractory WPW syndrome, has been replaced by catheter-based procedures. Compared with surgical techniques, catheter ablation has comparable success rates, lower mortality and complication rates, and improved cost-effectiveness. Moreover, newer catheter mapping systems now allow shorter procedure times. Surgical ablation, however, may be necessary in patients in whom catheter ablation has failed. Because this patient had a symptomatic tachyarrhythmia, he underwent electrophysiologic mapping followed by transvenous catheter ablation. He has remained asymptomatic since this procedure.
Patients with infrequent or minimally symptomatic arrhythmias may be treated pharmacologically. The aim of pharmacologic therapy is to alter the electrophysiologic properties, such as the refractoriness or conduction velocity of the AV node or the accessory bypass tracts.
Article taken from eMedicine March 2008

{kind=link}
{kind=link}